Most women with breast cancer have some type of surgery. Surgery is often needed to remove a breast tumor. Options for this include breast-conserving surgery and mastectomy. The breast can be reconstructed at the same time as surgery or later on. Surgery is also used to check the lymph nodes under the arm for cancer spread. Options for this include a sentinel lymph node biopsy and an axillary (armpit) lymph node dissection.
Breast-conserving surgery
This type of surgery is sometimes called partial (or segmental) mastectomy. It only removes a part of the affected breast, but how much is removed depends on the size and location of the tumor and other factors. If radiation therapy is to be given after surgery, small metallic clips (which will show up on x-rays) may be placed inside the breast during surgery to mark the area for the radiation treatments.
Lumpectomy removes only the breast lump and a surrounding margin of normal tissue. Radiation therapy is usually given after a lumpectomy. If adjuvant chemotherapy is to be given as well, radiation is usually delayed until the chemotherapy is completed.
Quadrantectomy removes more breast tissue than a lumpectomy. For a quadrantectomy, one-quarter of the breast is removed. Radiation therapy is usually given after surgery. Again, this may be delayed if chemotherapy is to be given as well.
If cancer cells are found at any of the edges of the piece of tissue removed, it is said to have positive margins. When no cancer cells are found at the edges of the tissue, it is said to have negative or clear margins. The presence of positive margins means that some cancer cells may have been left behind after surgery. If the pathologist finds positive margins in the tissue removed with surgery, the surgeon may need to go back and remove more tissue. This operation is called a re-excision. If the surgeon can't remove enough breast tissue to get clear surgical margins, a mastectomy may be needed.
The distance from the tumor to the margin is also important. Even if the margins are “clear”, they could be “close”—meaning that the distance between the edge of the tumor and edge of the tissue removed is too small and more surgery may be needed, as well. Surgeons can disagree on what is an adequate (or good) margin.
For most women with stage I or II breast cancer, breast-conserving surgery (BCS) plus radiation therapy is as effective as mastectomy. Survival rates of women treated with these 2 approaches are the same. But breast-conserving surgery is not an option for all women with breast cancer (see the section, "Choosing between breast-conserving surgery and mastectomy" below).
Radiation therapy can sometimes be omitted as a part of breast-conserving therapy. This is somewhat controversial, so women may consider BCS without radiation therapy if they are at least 70 years old and ALL of the following are true:
You should discuss this possibility with your health care team.
Possible side effects: Side effects of these operations can include pain, temporary swelling, tenderness, and hard scar tissue that forms in the surgical site. As with all operations, bleeding and infection at the surgery site are also possible.
The larger the portion of breast removed, the more likely it is that you will see a change in the shape of the breast afterward. If the breasts look very different after surgery, it may be possible to have some type of reconstructive surgery (see the section, "Reconstructive surgery"), or to have the size of the unaffected breast reduced to make the breasts more symmetrical. It may even be possible to have this done during the initial surgery. It's very important to talk with your doctor (and possibly a plastic surgeon) before surgery to get an idea of how your breasts are likely to look afterward, and to learn what your options might be.
Mastectomy

Mastectomy is surgery to remove the entire breast. All of the breast tissue is removed, sometimes along with other nearby tissues.
Simple mastectomy: In this procedure, also called total mastectomy, the surgeon removes the entire breast, including the nipple, but does not remove underarm lymph nodes or muscle tissue from beneath the breast. Sometimes both breasts are removed (a double mastectomy), often as preventive surgery in women at very high risk for breast cancer. Most women, if they are hospitalized, can go home the next day. This is the most common type of mastectomy used to treat breast cancer.
Skin-sparing mastectomy: For some women considering immediate reconstruction, a skin-sparing mastectomy can be done. In this procedure, most of the skin over the breast (other than the nipple and areola) is left intact. This can work as well as a simple mastectomy. The amount of breast tissue removed is the same as with a simple mastectomy.
This approach is only used when immediate breast reconstruction is planned. It may not be suitable for larger tumors or those that are close to the surface of the skin. Implants or tissue from other parts of the body are used to reconstruct the breast. This approach has not been used for as long as the more standard type of mastectomy, but many women prefer it because it offers the advantage of less scar tissue and a reconstructed breast that seems more natural.
A variation of the skin-sparing mastectomy is the nipple-sparing mastectomy. This procedure is more often an option for women who have a small early-stage cancer near the outer part of the breast, with no signs of cancer in the skin or near the nipple. In this procedure, the breast tissue is removed, but the breast skin and nipple are left in place. This is followed by breast reconstruction. The surgeon often removes the breast tissue beneath the nipple (and areola) during the procedure, to check for cancer cells. If cancer is found in this tissue, the nipple must be removed. Even when no cancer is found under the nipple, some doctors give the nipple tissue a dose of radiation during or after the surgery to try and reduce the risk of the cancer coming back.
There are still some problems with nipple-sparing surgeries. Afterward, the nipple does not have a good blood supply, so sometimes it can wither away or become deformed. Because the nerves are also cut, there is little or no feeling left in the nipple. In women with larger breasts, the nipple may look out of place after the breast is reconstructed. As a result, many doctors feel that this surgery is best done in women with small to medium sized breasts. This procedure leaves less visible scars, but if it isn't done properly, it can leave behind more breast tissue than other forms of mastectomy. This could result in a higher risk of cancer developing than for a skin-sparing or simple mastectomy. This was a problem in the past, but improvements in technique have helped make this surgery safer. Still, many experts consider nipple-sparing procedures too risky to be a standard treatment of breast cancer.
Modified radical mastectomy: This procedure is a simple mastectomy and removal of axillary (underarm) lymph nodes. Surgery to remove these lymph nodes is discussed in further detail later in this section.
Radical mastectomy: In this extensive operation, the surgeon removes the entire breast, axillary lymph nodes, and the pectoral (chest wall) muscles under the breast. This surgery was once very common, but less extensive surgery (such as modified radical mastectomy) has been found to be just as effective. This meant that the disfigurement and side effects of a radical mastectomy were not needed, so this surgery is rarely done now. This operation may still be done for large tumors that are growing into the pectoral muscles under the breast.
Possible side effects: Aside from post-surgical pain and the obvious change in the shape of the breast(s), possible side effects of mastectomy include wound infection, hematoma (buildup of blood in the wound), and seroma (buildup of clear fluid in the wound). If axillary lymph nodes are also removed, other side effects may occur (see the section, "Lymph node surgery").
Choosing between breast-conserving surgery and mastectomy
Many women with early-stage cancers can choose between breast-conserving surgery and mastectomy.
The main advantage of breast-conserving surgery (BCS) is that a woman keeps most of her breast. A disadvantage is the usual need for radiation therapy—most often for 5 to 6 weeks—after surgery. A small number of women having breast-conserving surgery may not need radiation while some women who have a mastectomy will still need radiation therapy to the breast area.
When deciding between BCS and mastectomy, be sure to get all the facts. You may have an initial gut preference for mastectomy as a way to "take it all out as quickly as possible." This feeling can lead women to prefer mastectomy even when their surgeons don’t. But the fact is that in most cases, mastectomy does not give you any better chance of long-term survival or a better outcome from treatment. Studies following thousands of women for more than 20 years show that when BCS can be done, doing mastectomy instead does not provide any better chance of survival.

Most women and their doctors prefer BCS and radiation therapy when it's a reasonable option, but your choice will depend on a number of factors, such as:
For some women, mastectomy may clearly be a better option. For example, breast conserving surgery is usually not recommended for:
Other factors may need to be taken into account as well. For example, young women with breast cancer and a knownBRCA mutation are at very high risk for a second cancer. These women often consider having the other breast removed to reduce this risk, and so may choose mastectomy for the breast with cancer as well. A double mastectomy may be done to treat the cancer and reduce the risk of a second breast cancer.
It is important to understand that having a mastectomy instead of breast-conserving surgery plus radiation only lowers your risk of developing a second breast cancer in the same breast. It does not lower the chance of the cancer coming back in other parts of the body. It is important that you don’t rush into making a decision, but instead take your time deciding whether a mastectomy or breast-conserving surgery plus radiation is right for you.
Lymph node surgery

To determine if the breast cancer has spread to axillary (underarm) lymph nodes, one or more of these lymph nodes may be removed and looked at under the microscope. This is an important part of staging and determining treatment and outcomes. When the lymph nodes contain cancer cells, there is a higher chance that cancer cells have also spread through the bloodstream to other parts of the body. The presence of cancer cells in the lymph nodes under the arm is often an important factor in deciding what treatment, if any, is needed after surgery (adjuvant therapy).
Axillary lymph node dissection (ALND): In this procedure, anywhere from about 10 to 40 (though usually less than 20) lymph nodes are removed from the area under the arm (axilla) and checked for cancer spread. ALND is usually done at the same time as the mastectomy or BCS, but it can be done in a second operation. This was once the most common way to check to see if breast cancer has spread to nearby lymph nodes, and it is still done in some patients. For example, an ALND may be done if a previous biopsy has shown one or more of the underarm lymph nodes have cancer cells.
Sentinel lymph node biopsy (SLNB): Although axillary lymph node dissection (ALND) is a safe operation and has low rates of most side effects, removing many lymph nodes increases the chance that the patient will have lymphedema after surgery (this side effect is discussed further on). To lower the risk of lymphedema, the doctors may use a sentinel lymph node biopsy (SLNB) procedure to check the lymph nodes for cancer. This procedure is a way of learning if cancer has spread to lymph nodes without removing as many of them.
In this procedure the surgeon finds and removes the first lymph node(s) to which a tumor is likely to drain. This lymph node, known as the sentinel node, is the one most likely to contain cancer cells if they have started to spread. To do this, the surgeon injects a radioactive substance and/or a blue dye into the tumor, the area around it, or the area around the nipple. Lymphatic vessels will carry these substances into the sentinel node(s).
A special device can be used to detect radioactivity in the nodes that the radioactive substance flows into or can look for lymph nodes that have turned blue. These are separate ways to find the sentinel node, but are often done together as a double check. The surgeon then cuts the skin over the area and removes the node(s) containing the dye (or radiation). A pathologist then looks closely at these nodes (often 2 or 3). (Because fewer nodes are removed than in an ALND, each one is looked at more closely for any cancer).
The lymph node can sometimes be checked for cancer during surgery. If cancer is found in the sentinel lymph node, the surgeon may go on to do a full axillary dissection. If no cancer cells are seen in the lymph node at the time of the surgery, or if the sentinel node is not checked at the time of the surgery, the lymph node(s) will be examined more closely over the next several days. If cancer is found in the lymph node, the surgeon may recommend a full ALND at a later time.
If there is no cancer in the sentinel node(s), it's very unlikely that the cancer has spread to other lymph nodes, so no further lymph node surgery is needed. The patient can avoid the potential side effects of a full ALND.
Until recently, if the sentinel node(s) had cancer cells, the surgeon would do a full ALND to see how many other lymph nodes were involved. But more recently, studies have shown that this may not always be needed. In some cases, it may be just as safe to leave the rest of the lymph nodes behind. This is based on certain factors, such as what type of surgery is used to remove the tumor, the size of the tumor, and what treatment is planned after surgery. Based on the studies that have looked at this, skipping the ALND may be an option for patients with tumors 5 cm (2 inches) or smaller who are having breast-conserving surgery followed by radiation. Because this hasn’t been studied well in women who have had mastectomy, it isn’t clear that skipping the ALND would be safe for them.
SLNB is done to see if a breast cancer has spread to nearby lymph nodes. This procedure is not done if any of the lymph nodes are known to contain cancer. If any of the lymph nodes under the arm or around the collar bone are swollen, they may be checked for cancer spread directly. Most often, a needle biopsy (either a fine needle aspiration biopsy or a core needle biopsy) is done. In these procedures, the surgeon inserts a needle into the lymph node to remove a small amount of tissue, which is then looked at under a microscope. If cancer cells are found, a full ALND is recommended.
Although SLNB has become a common procedure, it requires a great deal of skill. It should be done only by a surgeon who has experience with this technique. If you are thinking about having this type of biopsy, ask your health care team if they do them regularly.
Possible side effects: As with any operation, pain, swelling, bleeding, and infection are possibilities.
The main possible long-term effect of removing axillary lymph nodes is lymphedema (swelling) of the arm. Because any excess fluid in the arms normally travels back into the bloodstream through the lymphatic system, removing the lymph nodes sometimes blocks the drainage from the arm, causing this fluid to build up. This results in arm swelling.
Up to 30% of women who have a full ALND develop lymphedema. It also occurs in up to 3% of women who have a sentinel lymph node biopsy. It may be more common if radiation is given after surgery. Sometimes the swelling lasts for only a few weeks and then goes away. Other times, the swelling lasts a long time. Ways to help prevent or reduce the effects of lymphedema are discussed in the section, "What happens after treatment for breast cancer?" If your arm is swollen, tight, or painful after lymph node surgery, be sure to tell someone on your cancer care team right away. More information about lymphedema can be found in our document, Lymphedema: What Every Woman With Breast Cancer Should Know.
You may also have limited movement in your arm and shoulder after surgery. This is more common after an ALND than a SLNB. Your doctor may give you exercises to ensure that you do not have permanent problems with movement (a frozen shoulder). Numbness of the skin on the upper, inner arm is another common side effect because the nerve that controls sensation here travels through the lymph node area.
Some women notice a rope-like structure that begins under the arm and can extend down towards the elbow. This, sometimes called axillary web syndrome or lymphatic cording, is more common after an ALND than SLNB. Symptoms may not appear for weeks or even months after surgery. It can cause pain and limit movement of the arm and shoulder. This often goes away without treatment, although some patients seem to find physical therapy helpful.
Reconstructive surgery
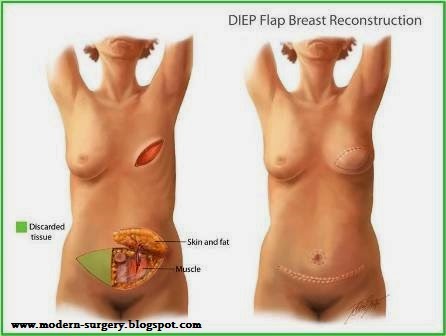
After having a mastectomy (or some breast-conserving surgeries), a woman might want to consider having the breast mound rebuilt; this is called breast reconstruction. These procedures are done to restore the breast's appearance after surgery.
If you are thinking about having reconstructive surgery, it is a good idea to talk about it with your surgeon and a plastic surgeon experienced in breast reconstruction before your cancer surgery. This will allow you to consider all reconstruction options. You’ll want your breast surgeon and your plastic surgeon to work together to come up with a treatment plan that will put you in the best possible position for reconstruction in case you decide to pursue it, even if you want to wait and have reconstructive surgery later.
Decisions about the type of reconstruction and when it will be done depend on each woman's medical situation and personal preferences. You may have a choice between having breast reconstruction at the same time as the mastectomy (immediate reconstruction) or at a later time (delayed reconstruction). There are several types of reconstructive surgery. Some use saline (salt water) or silicone implants, while others use tissues from other parts of your body (called an autologous tissue reconstruction).
To learn about different reconstruction options, see our document, Breast Reconstruction After Mastectomy. You may also find it helpful to talk with a woman who has had the type of reconstruction you might be considering. Our Reach To Recovery volunteers can help you with this. You can find out more about our Reach To Recovery program on cancer.org or by calling 1-800-227-2345.
Some things you can expect
For many, the thought of surgery is frightening. But with a better understanding of what to expect before, during, and after the operation, many fears can be relieved.
Before surgery: Usually, you meet with your surgeon at least a few days before the operation to discuss the procedure and your medical history. This is a good time to ask specific questions about the surgery and go over potential risks. Be sure you understand what the extent of the surgery is likely to be and what you should expect afterward. If you are thinking about breast reconstruction, ask about this as well.
You will be asked to sign a consent form, giving the doctor permission to perform the surgery. You might also be asked to give consent for researchers to use any tissue or blood that is not needed for diagnostic purposes. This may not be of direct use to you, but it may be very helpful to women in the future.
Ask your doctor if you will possibly need a blood transfusion. If the doctors think a transfusion might be needed, you might be asked to donate blood beforehand. If you do not receive your own blood, it is important to know that in the United States, blood transfusion from another person is nearly as safe as receiving your own blood.
You will probably be told not to eat or drink anything starting the night before the surgery.
You will also meet with the anesthesiologist or nurse anesthetist, the health professional who will be giving you the anesthesia during your surgery.
During surgery:
You will have an IV (intravenous) line put in (usually in a vein in your arm), which the medical team will use to give medicines that may be needed during the surgery. Usually you will be hooked up to an electrocardiogram (EKG) machine and have a blood pressure cuff on your arm, so your heart rhythm and blood pressure can be checked during the surgery.
General anesthesia (where you are asleep) is used for most breast surgery. The length of the operation depends on the type of surgery being done. For example, a mastectomy with axillary lymph node dissection will usually take from 2 to 3 hours.
After surgery: After your surgery, you will be taken to the recovery room, where you will stay until you are awake and your condition and vital signs (blood pressure, pulse, and breathing) are stable. How long you stay in the hospital depends on the type of surgery being done, your overall state of health and whether you have any other medical problems, how well you do during the surgery, and how you feel after the surgery. Decisions about the length of your stay should be made by you and your doctor and not dictated by what your insurance will pay, but it is important to check your insurance coverage before surgery.
In general, women having a mastectomy and/or axillary lymph node dissection stay in the hospital for 1 or 2 nights and then go home. However, some women may be placed in a 23-hour, short-stay observation unit before going home.
Less involved operations such as breast-conserving surgery and sentinel lymph node biopsy are usually done in an outpatient surgery center, and an overnight stay in the hospital is usually not needed.
You may have a dressing (bandage) over the surgery site that may wrap snugly around your chest. You may have one or more drains (plastic or rubber tubes) coming out from the breast or underarm area to remove blood and lymph fluid that collects during the healing process. You will be taught how to care for the drains, which may include emptying and measuring the fluid and identifying problems the doctor or nurse needs to know about. Most drains stay in place for 1 or 2 weeks. When drainage has decreased to about 30 cc (1 fluid ounce) each day, the drain will usually be removed.
Most doctors will want you to start moving your arm soon after surgery so that it won't get stiff.
How long it takes to recover from breast cancer surgery depends on what procedures were done. Most women can return to their regular activities within 2 weeks after a BCS with ALND, while recovery time is often shorter for BCS plus a SLNB. It can take up to 4 weeks after a mastectomy. Recovery time is longer if reconstruction was done as well, and it can take months to return to full activity after some procedures (for more information about recovery after breast reconstruction, please see our document Breast Reconstruction After Mastectomy). Still, these times can vary from person to person, so you should talk to your doctor about what you can expect.
Even after the doctor clears you to return to your regular level of activity, though, you could still feel some effects of surgery. You might feel stiff or sore for some time. The skin of your chest or underarm area may feel tight. These feelings tend to improve over time. Some women have problems with pain, numbness, or tingling in the chest and arm that continues for a long time after surgery. This, sometimes called post-mastectomy pain syndrome, is discussed in more detail later.
Many women who have breast-conserving surgery or mastectomy are often surprised by how little pain they have in the breast area. But they are less happy with the strange sensations (numbness, pinching/pulling feeling) they may feel in the underarm area.
Ask a member of your health care team how to care for your surgery site and arm. Usually, you and your caregivers will get written instructions about care after surgery. These instructions should include:
Most patients see their surgeon about 7 to 14 days after the surgery. Your doctor should explain the results of your pathology report and talk to you about the need for further treatment. If you will need more treatment, you will be referred to a radiation oncologist and/or a medical oncologist. If you are thinking about breast reconstruction, you may be referred to a plastic surgeon as well.
Chronic pain after breast surgery
Some women have problems with nerve (neuropathic) pain in the chest wall, armpit, and/or arm after surgery that doesn’t go away over time. This is called post-mastectomy pain syndrome (PMPS) because it was first described in women who had mastectomies, but it occurs after breast-conserving therapy, as well. Studies have shown that between 20% and 30% of women develop symptoms of PMPS after surgery. The classic symptoms of PMPS are pain and tingling in the chest wall, armpit, and/or arm. Pain may also be felt in the shoulder or surgical scar. Other common complaints include numbness, shooting or pricking pain, or unbearable itching. Most women with PMPS say their symptoms are not severe.
PMPS is thought to be linked to damage done to the nerves in the armpit and chest during surgery. But the causes are not known. Women who are younger, had a full ALND (not just SLNB), or who were treated with radiation after surgery are more likely to have problems with PMPS. Because ALNDs are done less often now, PMPS is less common than it once was.
It is important to talk to your doctor about any pain you are having. PMPS can cause you to not use your arm the way you should and over time you could lose the ability to use it normally.
PMPS can be treated. Opioids (narcotics) are medicines commonly used to treat pain, but they don't always work well for nerve pain. But there are medicines and treatments that do work for this kind of pain. Talk to your doctor to get the pain control you need.
No comments:
Post a Comment